
Could S-modafinil be the new caffeine?
S-modafinil is the shorter half-life enantiomer of modafinil

“If little white pills like Ritalin and Modafinil were dispensed as liquid in coffee cups, people would think about them in a very different way.” - Anders Sandberg
The idea of popping a “smart pill” and increasing your IQ and productivity is very alluring. Many young people fall prey to chasing this idea, rather than focusing on more sensible things like exercising, eating healthy, and sleeping better.
Indeed, I once fell into an obsession over nootropics and tweaking my nootropic stack in an attempt to make myself smarter.1 Needless to say, I ultimately concluded there is no pill that will raise your IQ, and virtually any substance you take is going to involve trade-offs.2 If there was a magical compound that made your brain smarter and more productive with no side-effects, evolution probably would have found it by now (the “Algernon argument”).
At the same time, there are many substances humanity has figured out how to use in useful ways. Alcohol works as a social lubricant, but it depresses cognition and comes with many health risks. Caffeine helps with morning alertness and accurately carrying out repetitive tasks, although at the expense of lower sleep quality and dependency. Nicotine (in its pure form) helps with a lot of aspects of cognitive function (see my 2017 post) but with the downside of dependency, addiction, and possible long-term health risks.3
There is a speculative argument that the relative consumption of these big three - alcohol, coffee, and nicotine - has had a profound effect on human societies and what they do. Malcomb Gladwell wrote about this in his essay “Java Man”, and Michael Pollan has written and spoken about this topic as well. Pollan notes how the Enlightenment and Scientific Revolution occurred concomitantly with a decline in alcohol consumption and a rise of caffeine and nicotine consumption. Regardless of whether one buys into the “caffeine and nicotine caused the Enlightenment” hypothesis, it is indisputable that caffeine aided industrialization by allowing assembly line workers to sustain focus longer on their work. Coffee breaks were invented for a reason.
Are there any other compounds out there that might have a transformative impact on par with alcohol, caffeine, and nicotine? This post explores s- enantiomer of modafinil, which is currently nearly unknown, as a possible candidate.

Why modafinil?
In a 2017 survey of /r/nootropics members, modafinil ranked third for “increasing motivation” after Adderall and Ritalin. In a 2020 survey of Astral Codex Ten readers, modafinil was the most highly rated nootropic, followed by caffeine and microdosing psilocybin. A 2022 survey by Troof found modafinil to be the fourth highest rated substance after dexedrine, adderall, and ritalin. Microdosing is a candidate for “potentially impactful substance”, however there’s a serious chance it’s all just an “active placebo” (you feel the subtle effects of it and get very excited — “it’s working!” — and then go do a bunch of work). An initial (N=20) randomized controlled trial on microdosing found no effects on mood or cognition. ADHD medications are obviously very useful to a subset of people, but for many non ADHD people they can cause overfocus. They also have abuse potential which means they are very unlikely to ever be fully legalized.
Modafinil has a number of properties that make it an excellent nootropic:
It promotes wakefulness.
Multiple studies show modafinil improves cognitive function.4
It is non-addictive and has zero abuse potential (unlike most other stimulants).
Modafinil has relatively limited side effects (discussed below).
It has a great safety profile, has been studied for decades, and no long-term negative effects are known.
It has mood-enhancing properties.
It may be neuroprotective.
Not surprisingly then, modafinil is increasingly preferred over amphetamines by militaries for keeping their soldiers awake and alert. Studies also suggest it can help doctors and surgeons do their work better. Admittedly the cognitive-enhancement properties of modafinil are still pretty overhyped - if you dig into the metanalysis on the subject, the gains, while statistically significant, are pretty small.
Why not modafinil?
There can be some serious downsides to modafinil use. First, it’s worth pointing out the modafinil’s drug-drug interactions. Modafinil is a weak inducer of the liver enzyme CYP3A, which means it can lower the effectiveness of things like birth control (ethinyl estradiol) and drugs like cyclosporine and quetiapine. It is also an inhibitor of CYP2C19, so it will increase the concentrations of drugs like diazepam, propranolol, and omeprazole, and to a lesser degree many antidepressants.
In Gwern’s “Modafinil Community Survey”, the four biggest side-effects reported were headache, smelly urine, insomnia, and anxiety/fast heart rate. Out of these, I think the sleep-disrupting effects of modafinil are the most problematic. Of course, I’m a bit biased here as this is the reason I personally can’t tolerate modafinil, but the problem seems pretty general. A big way that modafinil works is by stimulating the release of orexins and histamine, both of which are neurotransmitters that play an important role in the maintenance of circadian rhythm. Even among those who didn’t report insomnia as a side effect, there’s a good chance the quality of their sleep was diminished, but they didn’t realize it, especially if they were taking it daily. Modafinil does a really good job of masking poor sleep. Despite what nuts like Alexey Guzey may claim, for most people the negative effects of sleep disruption on cognition and productivity are quite large, at least in the early phases of taking it.
It is possible that the brain may adjust to modafinil within a ~week or so and the sleep disruption may subside (modafinil takes 2-3 days to reach steady-state concentration an generally compensatory genetic upregulation and downregulation takes a few days to a few weeks). To some extent sleep disruption can also be compensated for by simply taking a lower dose (eg 25-50 mg instead of 100 mg), which may actually be the optimal dose range for many people.5 In theory the wakefullness promoting effects of modafinil could be compensated for by taking an orexin antagonist and a sedating antihistamine before bed, but figuring out the precise dosing to achieve this well would be tricky, and tolerance to sedating antihistamines develops rapidly.
(added 1/16/23): Someone on Reddit pointed out that there’s a case report from the UK reported where someone developed a serious skin condition, Stevens-Johnson syndrome, after starting modafinil. As is typical, the case report garnered significant media coverage. Right now there’s just one, possibly two cases known out of millions of people who have taken modafinil. However, people identified as at high risk for SJS (to the extent this is possible for a rare disease like SJS) should probably not take at modafinil. It appears skin rashes are a known rare side effect of modafinil observed in initial clinical trials but 75% of cases have been in patients younger than 17.
Why S-modafinil?

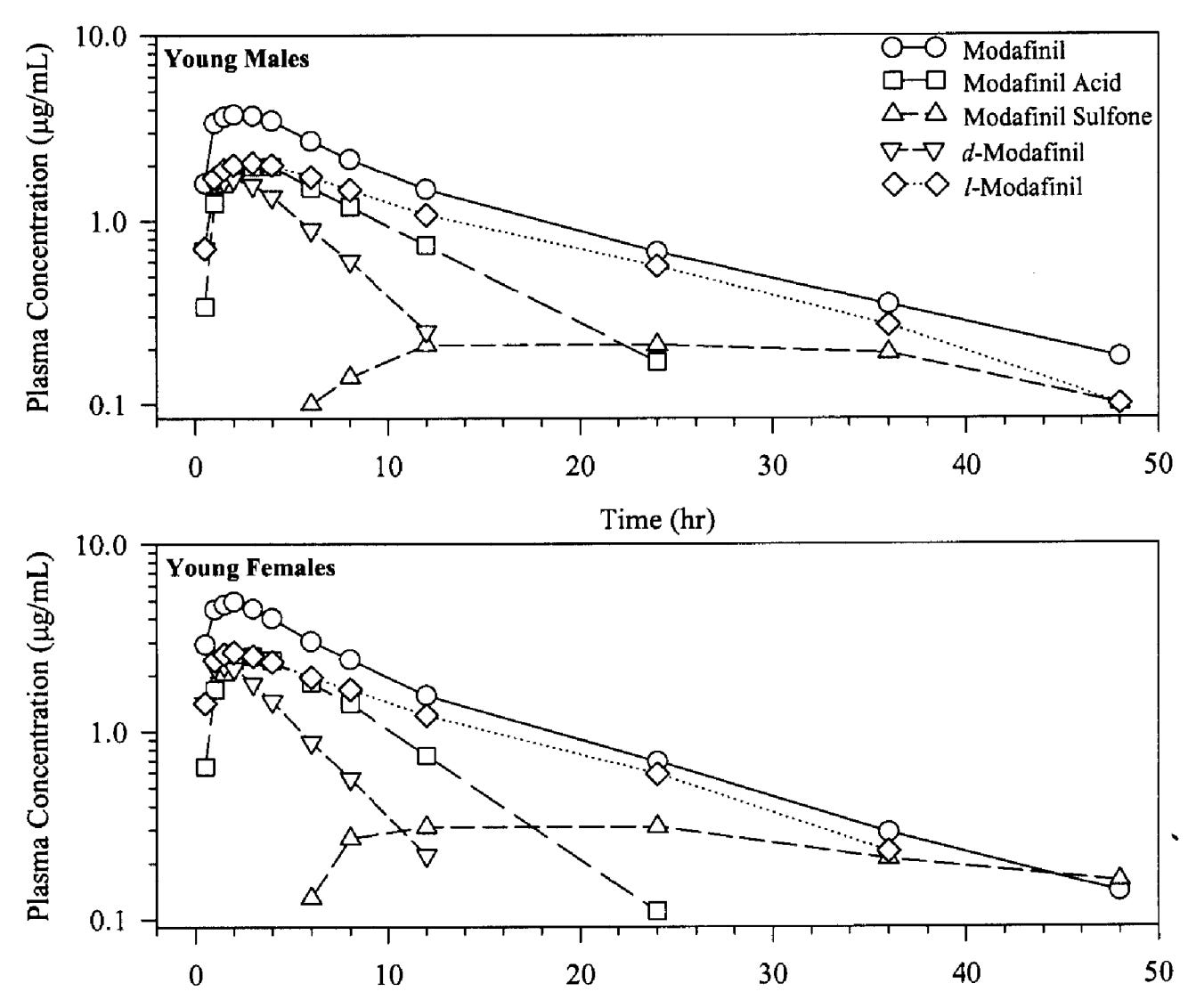
A fact that isn’t well appreciated is that modafinil comes in two chiral forms with different properties. The terminology used for these two forms varies, but most commonly they are known as R-modafinil (“armodafinil”) and S-modafinil (“esmodafinil”). Amazingly, S-modafinil has a much shorter half life! The half life of R-modafinil is 10 - 13 hours, rising to 14 - 16 hours when dosed daily. The half life of S-modafinil is only about 3 - 5 hours. This is similar to the half-life of caffeine!
The psychotropic properties of R-modafinil and S-modafinil appear to be somewhat different. In rats, S-modafinil binds to the dopamine transporter about 1/3 as strongly as armodafinil.6 This might actually be good (the abuse and addiction potential of modafinil are already quite low, but this indicates S-modafinil would have even lower abuse potential than R-modafinil or the racemic mixture). There is no other known drug with the combination of pharmacological and pharmacokinetic properties S-modafinil has.7 There are some studies that give S-modafinil to humans but I could find no experience reports for it anywhere online (if you actually somehow managed to try it, please comment below!).
Owing to its higher half life and potency, pure R-modafinil is FDA approved for “excessive daytime sleepiness associated with obstructive sleep apnea, narcolepsy, and shift work disorder” where it is sold as Nuvigil. It is difficult to synthesize pure R-modafinil and so during the synthesis some S-modafinil is created and just thrown out, rather than sold.8
Somewhat counter-intuitively, S-modafinil might actually help cure insomnia rather than cause it. One of the big factors that sustains insomnia is lack of activity and excessive napping during the day. People with very bad insomnia are so fatigued they don’t do much during the day and often nap several times. Unfortunately, this leads to a lack of sleep drive and poorer sleep the next night, leading to a vicious cycle. Modafinil has been studied as a way to keep insomniacs awake during the day in hopes they might sleep better the next night. Unfortunately it isn’t well suited for this task because of its long half life, but S-modafinil might be. Despite its long half life, R-modafinil is FDA approved for the normalization of sleep-wake patterns in people with shift-work disorder. One wonders if S-modafinil might have been a better choice!
Will this ever happen?
“De-scheduling a drug in the United States is a long and arduous process, but given the benefits of legalizing modafinil, the struggle could be worth it.”
— Daniel Oberhaus, “Why Can't We All Take Modafinil?”
Unfortunately, modafinil is a schedule IV controlled substance in the US. This absurd scheduling puts it in the same category as aphetamines and benzodiazapines, even though many studies show modafinil has zero abuse potential. In other countries like the UK, Australia, India, Germany, and Canada, modafinil is prescription-only but is not a controlled substance.
I suspect the first step to making S-modafinil available would be to get a pharmaceutical company to study it for the treatment of some disease, and then get it approved. Then at least it would be obtainable via prescription. Some conditions where S-modafinil might be useful are depression, ADHD, shift work sleep disorder, chronic fatigue syndrome9, fatigue from fibromyalgia, and fatigue from cancer/chemotherapy. Unfortunately, S-modafinil would likely fall under the same scheduling as R-modafinil, so the next step would be change this scheduling. Because of the interactions with birth control medications, full legalization may be difficult, unfortunately.
What would a world with widely available esmodafinil look like?
It’s really hard to know. Anecdotally, modafinil is reported to increase people’s productivity by increasing motivation and “grit”. It seems to increase processing speed slightly, increase focus, and make people more confident and agentic as well. I personally think a lot of this is pure expectation and placebo effects. Still, I think there is potential for S-modafinil to be transformative, otherwise I wouldn’t have written this post. Some preliminary research suggests that modafinil may help people with lower IQ more than people with higher IQ. Given that differences in IQ explain a lot of income inequality, could cheap and widely available S-modafinil help reduce inequality?
(Update 9-7-23: I finally met someone who has tried S-modafinil. They said it was “Ritalin-like” with a quick come-up, intense few hours of action, and then a bit of a crash afterwards. This fits well with the research in rats suggesting it boosts dopamine more than R-modafinil.)
See a 2010 post I wrote on energy drink ingredients. At the time I was allured by the idea of nootropics and remained so for several years, experimenting with many of them. In the ends, the only substances I found consistently useful were caffeine and nicotine. Today the only nootropic or arguably-nootropic things I take are caffeine, fish oil, and a choline supplement.
See Gwern’s classic post “The Algernon Argument” and Scott Alexander’s post “Cognitive Enhancers: Mechanisms and Tradeoffs”. Also, see Gwern’s meticulous self-experiments on popular nootropics, most of which only small effects. I haven’t read all of Gwern’s stuff but it appears the only two things he found consistently helpful were modafinil and nicotine (he wrote lengthy disquisitions on both).
The risks of nicotine are generally over-stated in many health articles online. It’s not even entirely the degree to which nicotine drives smoking addiction (nicotine replacement therapy doesn’t work that well). See Gwern’s review of health issues from nicotine.
Battleday, R. M., and A. K. Brem. “Modafinil for Cognitive Neuroenhancement in Healthy Non-Sleep-Deprived Subjects: A Systematic Review.” European Neuropsychopharmacology, vol. 25, no. 11, Nov. 2015, pp. 1865–81.
See the Yerkes-Dodson law, which states that task performance increases with physiological arousal, but only up to a point, after which it decreases. This is something to bear in mind when reading studies on the nootropic effects of modafinil which typically use a large fixed dose (100 mg, 200 mg, or even 400 mg). I suspect such large standard doses, while useful for conditions like chronic fatigue or narcolepsy, are likely too large for many people when it comes to optimizing cognitive function and productivity. This, combined with the huge genetic differences in drug metabolism that exist between people, mean the potential for modafinil as a productivity enhancer may be underestimated in such studies. Each person should figure out the best dose for themselves.
Loland, C. J., Mereu, M., Okunola, O. M., Cao, J., Prisinzano, T. E., Mazier, S., … Newman, A. H. (2012). R-Modafinil (Armodafinil): A Unique Dopamine Uptake Inhibitor and Potential Medication for Psychostimulant Abuse. Biological Psychiatry, 72(5), 405–413.
I searched for a while and also consulted with Matthew Baker, a nootropics expert. The closest thing I could find to S-modafinil is fluorenol (also called hydrafinil, although this is a misnomer because its structure is quite different from afinil compounds). Various sources online say fluorenol has a half life somewhere in the 6-8 hours range. Fluorenol is toxic in aquatic animals and its safety in humans has not been well-established.
The process by which Cephalon synthesizes R-modafinil is described in Hauck, W., Adam, P., Bobier, C., & Landmesser, N. (2008). Use of large‐scale chromatography in the preparation of armodafinil. Chirality, 20(8), 896–899.
The process uses preferential crystallization of the S-enatiomer of modafinic acid and high pressure liquid chromatography. (see description here). For cost-reduction reasons they try to avoid making S-modafinil as much as possible, but do make some in the early stages of the process.
A 2005 (N=14) RCT on the use of modafinil for CFS/ME found it didn’t help, but there are case reports where modafinil (sometimes combined with CBT) either improved or completely cured CFS/ME. Notably, in the 2005 study three patients (18%) dropped out due to side effects including insomnia. It’s possible that the high doses of modafinil (200 mg - 400 mg) used in the study resulted in poorer quality sleep which negated the helpful aspects of modafinil. S-modafinil is less likely to have caused the insomnia that was experienced.
When I took modafinil 15 or 20 years ago, it made me itch terribly. More recently when I took it, that wasn't an issue but greatly increased problems with my chronic phlegm issue. Also, it focuses me, but not necessarily on what I need to be focused on! I concluded that it's not for me.
You're correct that modafinil does have a history of generally safe clinical use. That said, you should include reports of harmful skin reactions such as Stevens-Johnson syndrome. They were the reason why modafinil was not approved by the FDA for ADHD. More recently, harmful skin reactions were part of why the European Medicines Agency restricted modafinil's approved uses.